
On February 15, 2024, the Clock Foundation’s Executive Director, Bobby Brooke, led an inaugural session of Longevity Connect. The aim of this session was to sift through the deluge or “firehose” of new information that is flooding the longevity field and highlight key papers and findings that have emerged in the last few weeks and months.
Along with covering the launch of our first longevity open enrollment group dedicated to AKG (excluded here for brevity), Brooke reviewed recent mechanistic studies, provided an overview of the newest findings from leading aging researchers and influencers, and discussed the latest in aging research initiatives. His presentation also covered a range of treatment papers, revealing the latest therapeutic approaches and general interest topics within the rapidly evolving field of longevity science.
Below is the full video presentation, full citations, screenshots and transcript.
Agenda and Table of Contents of Topics Covered
1. ⏰ Review of Epigenetic Clock Papers
2. ???? Mechanistic study review – Information Theory of Aging, B12 Reprogramming, etc.
3. ???? Aging biomarkers review – Aging Hallmarks, Future: Wearables, Early detection
4. ???? Treatment Papers & News – Rapamycin, TLR5
5. ???? Influencer & Initiative Updates ???? – RMR , MMC , ITP , Blueprint (BJ), Attia (PA), Sinclair (DS), etc. – Test their protocols?6. ????️Twitter Talk: Has anyone ever really reversed aging? ????
About Us:
Founded by Steve Horvath and Bobby Brooke, the nonprofit Clock Foundation (https://clockfoundation.org) is dedicated to pushing the boundaries of longevity research for tangible improvements in human health and lifespan. We’ve completed over 300 longevity projects in our first 3 years. We offer cutting-edge biological age testing and a range of longevity services and software solutions for individuals and groups (clinics, researchers and coaches) interested in quantifying aging and managing anti-aging programs, intervention studies and trials. Learn more at https://clockfoundation.org/get-started/. Buy your first biological age test at MyAgingTests.com.
Longevity Connect is a Monthly Longevity Science and Anti-Aging Strategies Virtual Meetup, brought to you by Clock Foundation and MyAgingTests.com.
Got questions or interested in joining our next Longevity Connect event? Check our event schedule and signup at https://myagingtests.com/longevity-connect/.
Disclaimer
Disclaimer: Nearly all aging biomarker tests today are “research use only” tests, which means they are not approved by FDA for use in treatment of any diseases. There is no guarantee that even with the best measures of biological or epigenetic age, i.e. epigenetic clocks, that if you reverse it by 5 years it will always translate into 5 extra years of life.
You should always consult your physician before initiating any new treatment.
Conflicts of Interest: I (Bobby Brooke) work with a private biotech company Intervene Immune developing treatments for immune system regeneration. Through Clock Foundation I work as a non-profit collaborator for dozens of aging researchers, including many academics and longevity biotech companies.
For Longevity Connect recaps, we focus on analysis of data that’s already been published, and largely on treatments that are already available for use in clinical trials.
Key Topics: Longevity Connect on Feb 15, 2024
⏰ Epigenetic Clock Papers – Clock Tech
One of the core technologies we leverage at the Clock Foundation are Epigenetic Clocks, so we take a keen interest in development of new clocks, clock components and ways to decrease cost of testing.
Here are a few key updates centered on “Clock Tech”:
Causality-enriched clocks uncouple damage & adaptation – Gladyshev, MR:
Machine learning models based on DNA methylation data can predict biological age but often lack causal insights. By harnessing large-scale genetic data through epigenome-wide Mendelian randomization, we identified CpG sites potentially causal for aging-related traits. Neither the existing epigenetic clocks nor age-related differential DNA methylation are enriched in these sites. These CpGs include sites that contribute to aging and protect against it, yet their combined contribution negatively affects age-related traits. We established a new framework to introduce causal information into epigenetic clocks, resulting in DamAge and AdaptAge—clocks that track detrimental and adaptive methylation changes, respectively.
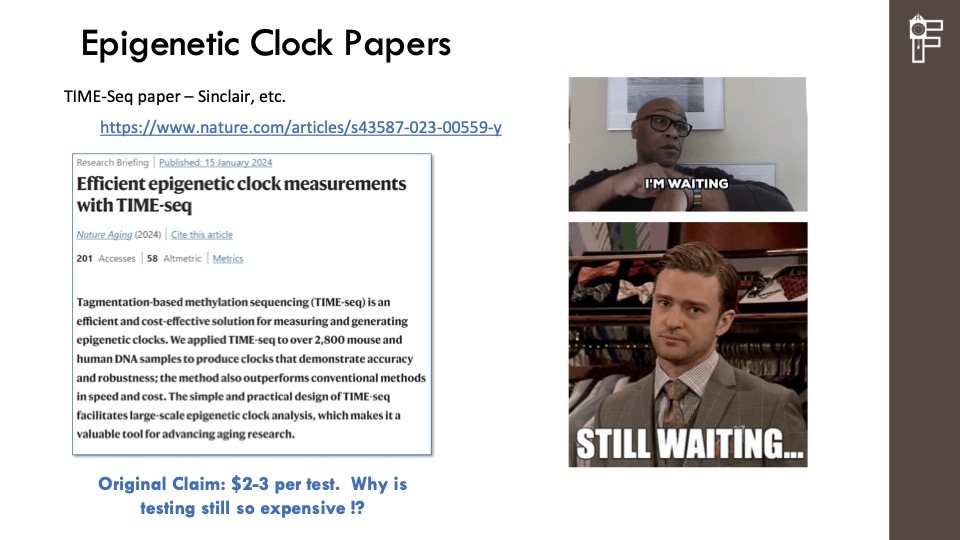
TIME-Seq paper – Sinclair, Gladyshev, etc.
A new, extremely low-cost methylation testing method has been proposed by Sinclair and associates. If it works it claims to offer testing at $2-3 per test. But we are still waiting to validate:
Full List of papers reviewed:
- Causality-enriched clocks uncouple damage & adaptation – Gladyshev, MR https://www.nature.com/articles/s43587-023-00557-0
- Comprehensive map of ageing blood methylome – Eynon et al, 32K blood samples https://www.researchsquare.com/article/rs-3755475/v1
- RESNet Age – Changchun University, China – Public data & neural net ML https://www.mdpi.com/2306-5354/11/1/34
- Biologically informed methods for deep learning explainable clocks – XAI-AGE https://www.nature.com/articles/s41598-023-50495-5
- Saliva-based methods – explainable, with protein EpiScores scores – Multi-omic MRS https://www.biorxiv.org/content/10.1101/2023.12.21.572866v1
- TIME-Seq paper – Sinclair, Gladyshev, etc. – Low-cost methylation testing https://www.nature.com/articles/s43587-023-00559-y
???? Mechanisms of Aging Review
Mechanistic studies is a big part of the kind of studies we do, not only just to test new treatments but also to look at the biology of aging. This helps inform us about if we really understand the biology of aging and hopefully, that’s going to enable us to develop more and more effective treatments.
Here are a few notable papers that helps us understand the potential mechanism of biological aging:
Vitamin B12 emerges as key player during cellular reprogramming:

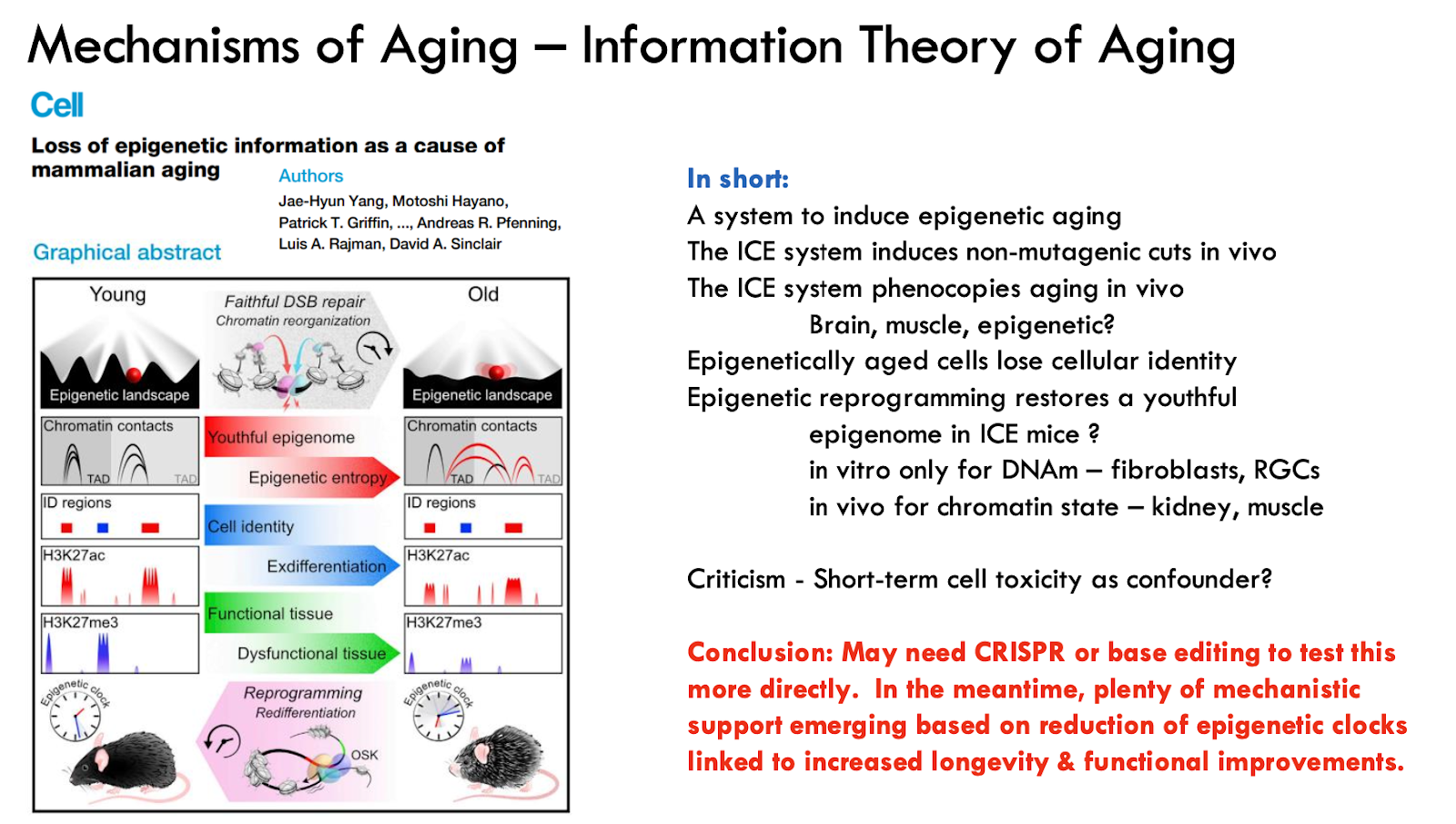
Information Theory of Aging on ICE Mice Model
Full list of papers reviewed:
- Vitamin B12 emerges as key player during cellular reprogramming https://www.nature.com/articles/s42255-023-00917-5
- Vitamin B12 is a limiting factor for induced cellular plasticity and tissue repair https://www.nature.com/articles/s42255-023-00916-6
- In vivo reprogramming leads to premature death linked to hepatic and intestinal failure (with silver lining shown at right) https://www.nature.com/articles/s43587-023-00528-5
- Information Theory of Aging https://www.nature.com/articles/s43587-023-00527-6
- Loss of epigenetic information as a cause of mammalian aging – https://www.cell.com/cell/fulltext/S0092-8674(22)01570-7
- Retroviral link to vertebrate myelination through retrotransposon RNA-mediated control of myelin gene expression https://www.repository.cam.ac.uk/items/0ba80aa0-6887-447b-8124-fe2292b50850
- Glial senescence enhances α-synuclein pathology owing to insuf. clearance by autophagy dysfunction https://www.nature.com/articles/s41420-024-01816-8
???? Aging biomarkers review and news ????⚕️
Longevity researcher Judy Campisi (b. 1948) recently passed away and we wanted to highlight her work this month, specifically

Lecot P, Alimirah F, Desprez P-Y, Campisi J, Wiley C. Context-dependent effects of cellular senescence in cancer development. Br J Cancer 2016;114:1180–4.
Wang B, Kohli J, Demaria M. Senescent Cells in Cancer Therapy: Friends or Foes? Trends in Cancer
2020;6:838–57. https://doi.org/10.1016/j.trecan.2020.05.004.
???? Treatment News ????????⚕️
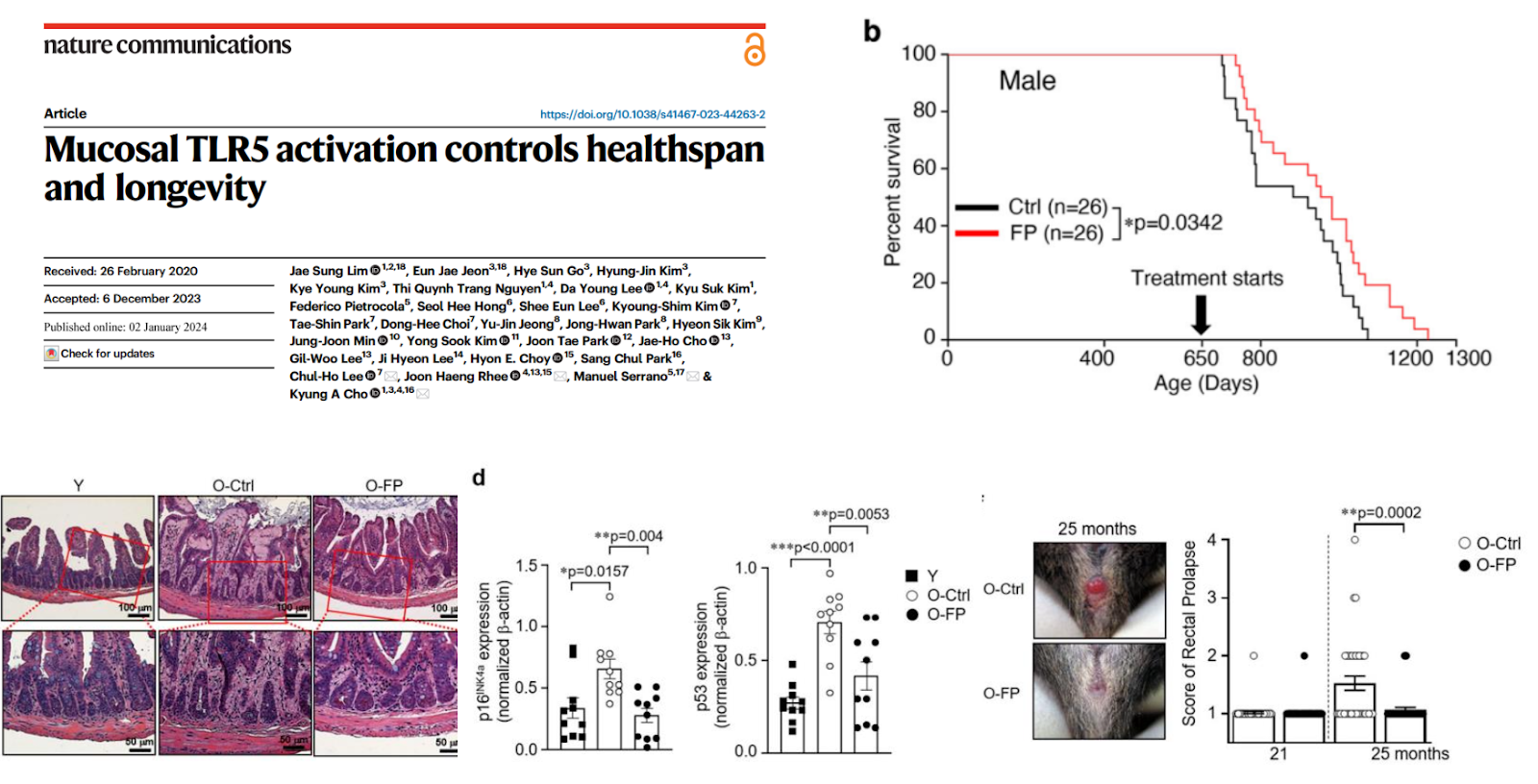
A few years ago some evidence came out about immune stimulation through TLR5 that can extend lifespan. We were excited to see a new paper in Nature titled: Mucosal TLR5 activation controls healthspan and longevity:
Rapamycin is one of the most talked about and promoted options for longevity pursuers and treatments. Check out Evaluation of off-label rapamycin use to promote healthspan in 333 adults for some newly reported benefits and side effects.

???? Influencer & Initiative Updates ????
From the “firehouse” of longevity news and researcher, here are a few areas were are watching and wanted to highlight:
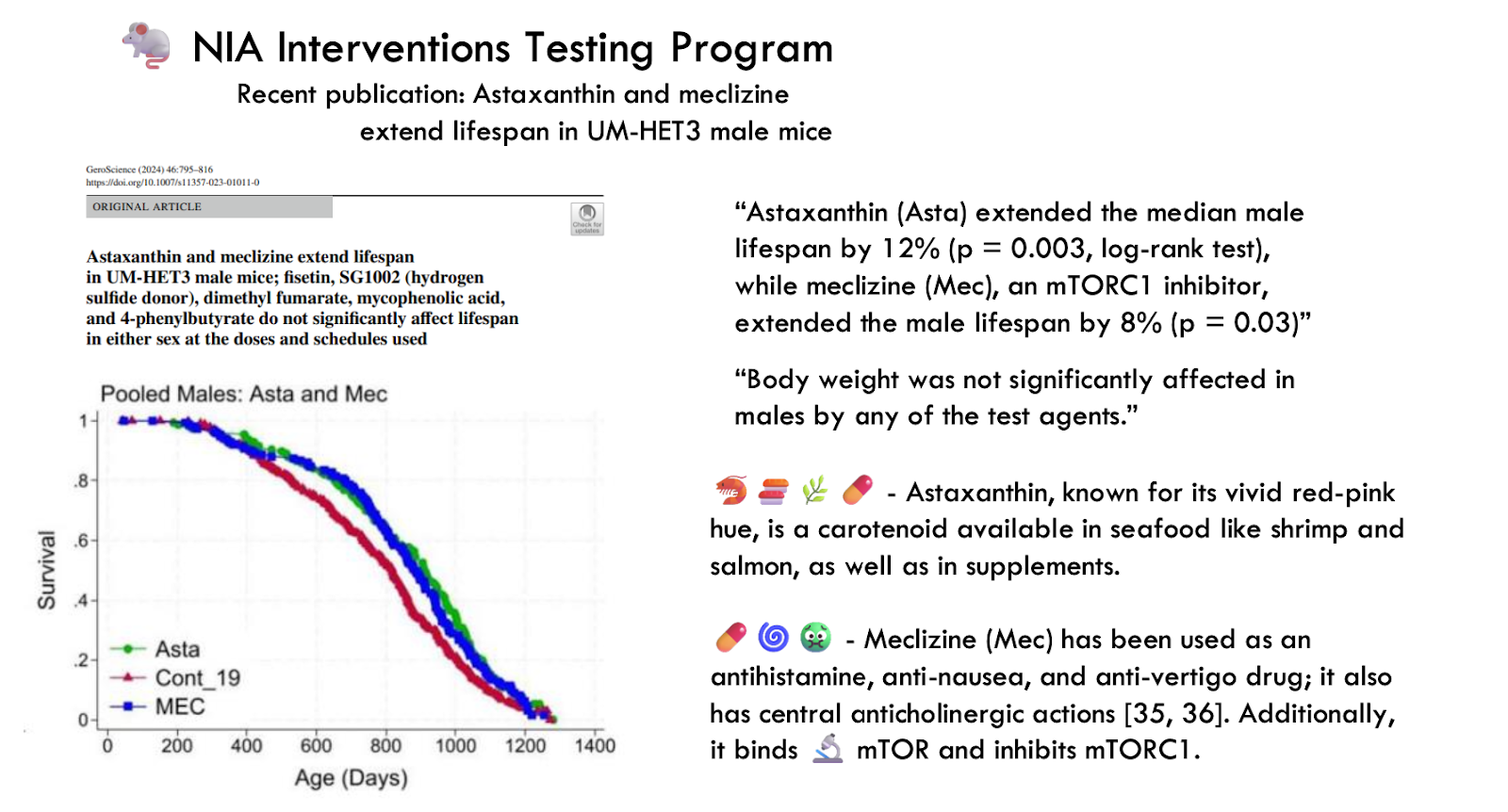
- “Astaxanthin (Asta) extended the median male lifespan by 12% (p = 0.003, log-rank test), while meclizine (Mec), an mTORC1 inhibitor, extended the male lifespan by 8% (p = 0.03)”
- “Body weight was not significantly affected in males by any of the test agents.”
- Astaxanthin, known for its vivid red-pink hue, is a carotenoid available in seafood like shrimp and salmon, as well as in supplements.
- Meclizine (Mec) has been used as an antihistamine, anti-nausea, and anti-vertigo drug; it also has central anticholinergic actions [35, 36]. Additionally, it binds mTOR and inhibits mTORC1.
???? Aubrey de Grey’s Robust Mouse Rejuvenation (RMR) Update:
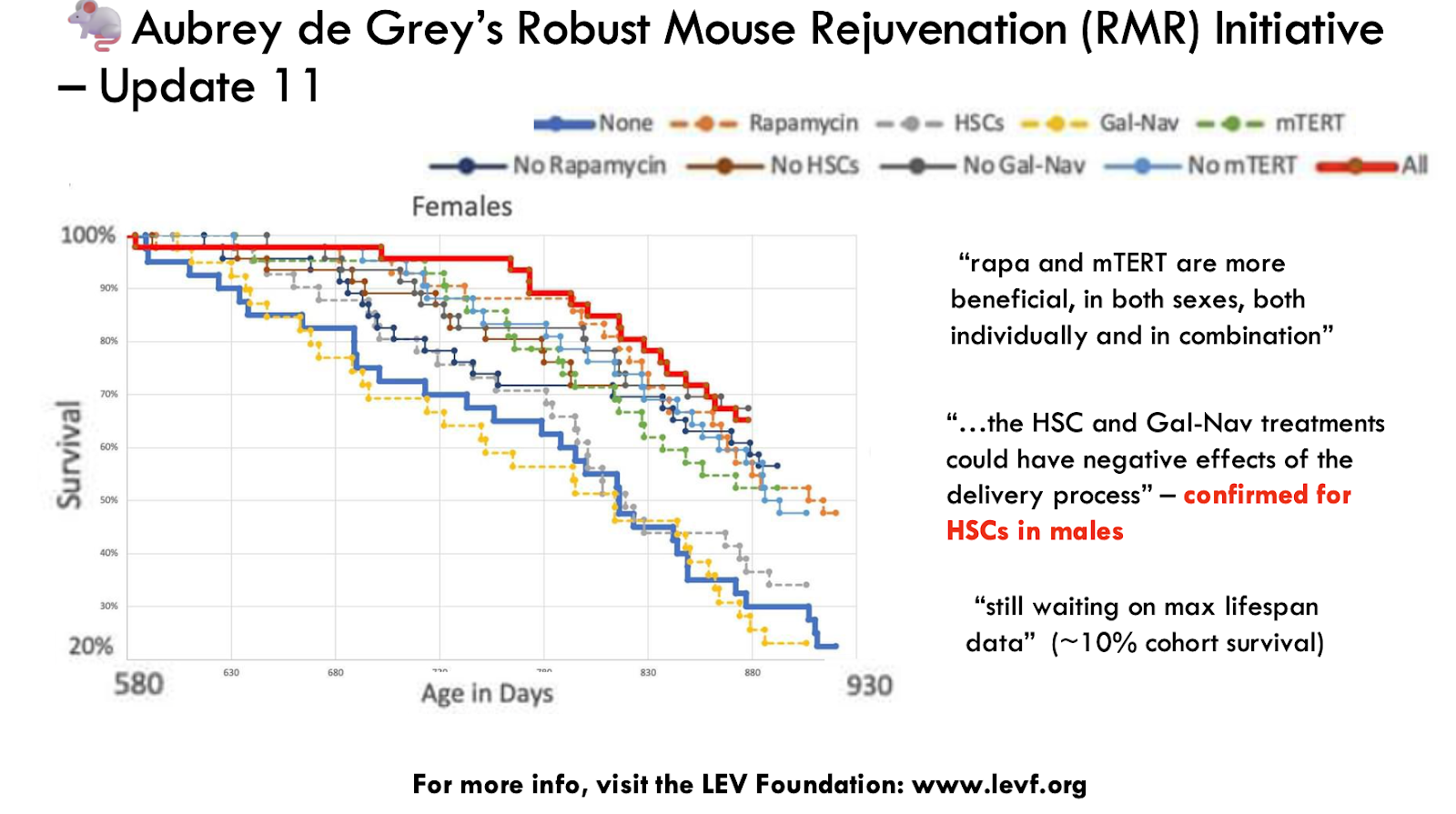
For more info, visit the LEV Foundation: www.levf.org.
Full list of notable updates:
- Aubrey de Grey’s Robust Mouse Rejuvenation Update #11
- Million Molecule Challenge (MMC) – sponsored by Ora Biomedical
- Efficient testing of drugs & combos in worms
- NIA Interventions Testing Program –
- New publication: Astaxanthin and meclizine
- extend lifespan in UM-HET3 male mice
- Peter Attia Podcast & Blogs – Cancer screening, Immunotherapy,
- Microbiome, Metabolic health & GLP-1, and more
- Bryan Johnson’s Blueprint – Launch of Blueprint Store,
- “Snake Oil” EVOO, New hire for memes, lots of comedy
- A4LI Regulatory Initiative – Upcoming DC Meet-up including Fortnoy, Kaeberlein, etc.
- XPRIZE Foundation’s launch of $101 million XPRIZE Healthspan
- 7-year global competition focused on >10 year improvement in function
????️Twitter Talk: Has anyone ever really reversed aging? ????
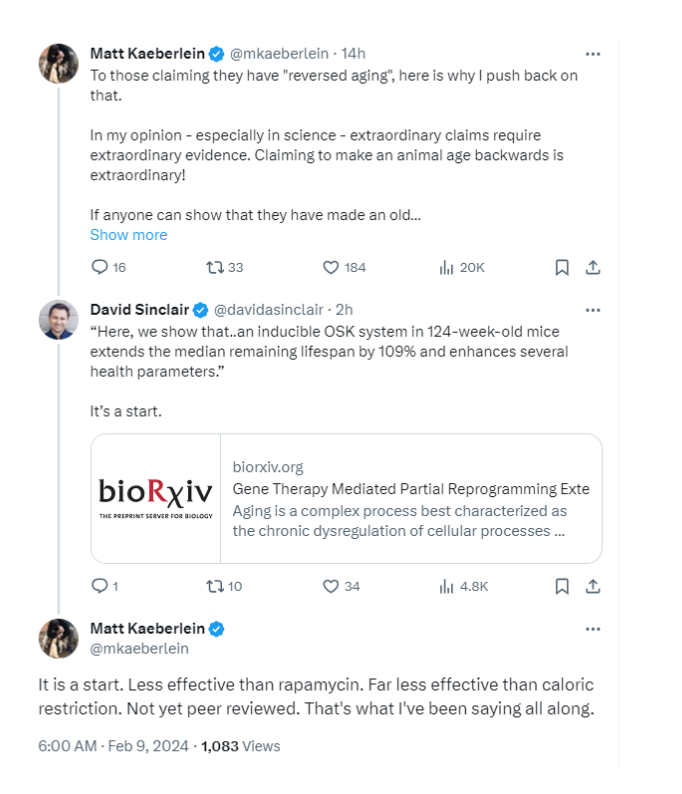
- Matt Kaeberlein: No, but max lifespan has increased by 25% with rapamycin, and up to 60% with old experiments and caloric restriction.
- David Sinclair: Quoted results from a new systemic OSK reprogramming system in mice (work done by Rejuvenate Bio and epigenetic testing by Clock) has extended REMAINING lifespan by 109% over controls. It’s a start.
Full Transcript (Revised for Clarity and Readability)
In this month’s Longevity Connect, I’ll take a look at recent epigenetic clock papers, review some mechanistic studies, and examine some “news” that’s coming out from influencers, from prominent aging researchers, and also from prominent aging research initiatives. And I’ll look at some treatment papers and also a couple of other general interest topics.
Mechanistic studies is a big part of the kind of studies we do, not only just to test new treatments but also to look at the biology of aging. This helps inform us about if we really understand the biology of aging and hopefully, that’s going to enable us to develop more and more effective treatments.
There is a flood of new information that’s coming out in the longevity field. So, a lot of what I’m talking about today are papers that have emerged in the last few weeks or maybe the last two months. What we intend to do is kind of harness that information and make the most of it and try to design the most effective treatments and studies of them.
First, I’ll look at some epigenetic clock papers that have all come out in the last couple of months.
One analogy that I’ve heard Steve Horvath mention a few times is that epigenetic clocks are somewhat like iPhones in that you’re going to have all of these different versions or kinds that are coming out. And, you know, and so there are different kinds of categories here.
The first is an exciting paper that Steve was a part of on causality enriched clocks. So they’re looking to find kind of CPGs or methylation sites that seem to be more drivers of aging rather than kind of downstream effects. There are papers that look at and they kind of characterize in large samples what’s kind of the locations of different methylation sites that are in epigenetic clocks. And then there are kind of a few kinds of, you know, I would say they’re kind of new iterations or new versions of clocks that are available. And so, for instance, this ResNet age paper came out where, similar to what Steve did in 2013, it looked at publicly available data on geo and they developed a multi-tissue clock for it. This was based on a different machine learning method. They used neural nets, but they developed a pretty accurate multi-tissue clock with it.
In these next two papers, these are kind of themes that I would say build on a lot of what, you know, what has been done with GrimAge and with GrimAge2. And there’s kind of in both of these papers, there’s this mention of having explainable clocks. And that’s a big focus for us is making your epigenetic clock results explainable, kind of interpretable, and then actionable, and where you can actually kind of personalize treatment and do something about it, you know, with your patients or with people in a study. And so GrimAge already does that to a significant extent. There are different components, and now if you haven’t seen them, we have systems aging reports that are available where we map each of the GrimAge components to a specific tissue or physiological system, and then you can target treatment for that component. And so a couple of groups have done that with, and they’ve done something similar with, and this one looking also at saliva samples, which is another advantage of GrimAge2, in that it’s more accurate with saliva samples, so it can be used with either blood or saliva.
The last paper here I’ll mention is this TimeSeq paper. You know, there was work, and that’s on a low-cost methylation technology from the Sinclair lab from a Harvard group. And, you know, this one is, so this is TimeSeq technology, and this was released on BioRxiv, I believe, a couple of years ago, and it led to a lot of attention for it because the kind of promise is that it could be a very inexpensive technology. Methylation testing today is a couple of hundred, you know, $200 to $300 per sample, and this was talking, you know, a couple of orders of magnitude less, down to $2 or $3 per test potentially.
But kind of the frustration is that it’s not, you know, is that it’s not available quite yet. We, you know, we are waiting. You know, we’re working on similar technologies as well. I mean, I really commend the group for, these groups for working on it. There probably are some drawbacks to the technology today, and that it doesn’t profile the entire epigenome. It may only end up profiling a thousand sites or a few thousand sites, and there is still a lot of work to be done to ensure that it’s really kind of reliable data that’s available from it. But we are hoping that technology like this will become available. You know, it’s not available quite yet. We are waiting. And we also have kind of separate initiatives with groups where before long, we believe methylation testing will come down pretty significantly in price. So maybe by the end of this year, it’ll be cut in half. But, you know, this type of technology could bring it down even more. I mean, there still are costs involved with like kits that are involved, the blood collections, the staff time for processing them. So two to three dollars probably is not reasonable. But, you know, under a hundred dollars for a methylation test that’s very reliable and comprehensive. I think that’s very much in our future. And it may be maybe a couple of years, but it will be available pretty before too long.
Here are some papers on mechanisms of aging. So these studies try to interrogate different aspects of the aging process and different aging hallmarks.
So there are a couple that are related to reprogramming and a group that looked at B12, vitamin B12, and its role in reprogramming. There was a study that we were a part of, you know, a small part of, you know, with on in vivo reprogramming. And it’s got kind of a scary title where in vivo reprogram leads to premature death due to hepatic and intestinal failure. But there is a silver lining with it.
Here’s a survival curve from it, because what they were able to do is to is to turn off OSKM to turn off the reprogramming factors in the organs that were that were linked to mortality. So turn them off in the liver and in the intestines. And it dramatically improved survival. It made it made in vivo reprogramming a lot safer. So so it was a quite promising result. There was work from the Sinclair lab on the information theory of aging. So a paper that came out on the loss of genetic information as a cause of mammalian aging. We’ll look at that paper. There’s a couple at the bottom that that I personally find interesting. They’re about brain aging and the role of myelin and remyelination.
I also find kind of the last one interesting. And just in general, with these mechanistic studies, often what they’re doing is they’re they’re kind of linking together different hallmarks of aging and helping understand how they interact and what’s more upstream versus downstream. And kind of the last paper here I found interesting because it is looking at glial senescence and then also kind of the role of autophagy there. And, you know, and, you know, I’m not going to review that in great detail. But in general, these are the types of studies that will profile ones that are examining multiple hallmarks of aging and determining how they interact.
In this paper from Manuel Serrano’s lab, looked at B12 in the role of reprogramming. And this was, you know, I thought interesting in that, I mean, it is just a mechanistic study, mostly in vitro, some in vivo data, but it’s using vitamin B12. And it’s also looking at SAM or SAMe, another widely available supplement and showing that they really have a profound effect on reprogramming and doubling or tripling the efficiency. And with very clear kind of unequivocal data, I mean, it’s a really elegant mechanistic or kind of elegant, exhaustive kind of mechanistic study. And to me, it’s inspiring and that these are agents that are available right now. They’re widely available, very inexpensive. This is not some new chemical entity that it’s going to take 10 years to develop and to have available for clinical trials. You know, these types of tools are available. We just need to better understand how to apply them.
And here’s a paper on, this is from the Sinclair lab, on the information theory of aging. And I think he’s written quite a bit about this in a book. And, but, you know, so this is a mouse model. It’s called the ICE system. And it is where it’s intended to induce epigenetic aging. And it, I believe it involves double strand breaks. And when it’s repaired, there are changes to methylation that appear to resemble kind of what happens with normal aging. And over time, your cells lose their identity. They lose that kind of fine-tuned control of their state. And then they were ultimately able to show in this paper through some amount of in vitro data and a little bit of in vivo data that some of those epigenetic changes were able to be reversed. And that was through reprogramming. And, you know, I mean, we were not involved in that study. And like the, you know, that,
you know, we’ve done a lot of preclinical studies, like I mentioned, over 200 preclinical projects. But, you know, this was not one of them that I’m aware of. I don’t think we’ve done kind of mammalian array work, you know, with the ICE mouse. I think that would be an exciting project. But so, I mean, and I think it would help us kind of characterize if this is really, if this model really kind of resembles epigenetic aging or, you know, the way we kind of see it across many studies.
And there has been some criticism from people about, you know, Charles Brenner, you know, who’s often critical of David Sinclair about kind of the model and about, you know, whether or not there’s short-term cellular toxicity in it that, you know, basically it’s kind of critical of the model in general, and in saying there’s a lot of genotoxicity and that maybe it doesn’t, in fact, kind of resemble kind of normal epigenetic aging. I think that’s still to be determined. I mean, maybe there are better models. I’m sure there will be better models emerging in the future like CRISPR or with base editing, that’s where you’re able to modify specific sites of the epigenome. I’m sure there will be better progeria-accelerated aging models of epigenetic aging. But for now, no, it seemed like a decent model. And there is also a lot of data that shows that epigenetic aging can be reduced based on treatments. And there’s a lot of data emerging that it’s been linked to functional improvements, but it is kind of early days. But overall, you know, I found it to be a pretty exhaustive and well-done study. It would have been, you know, I’m sure there’ll be more done with this model.
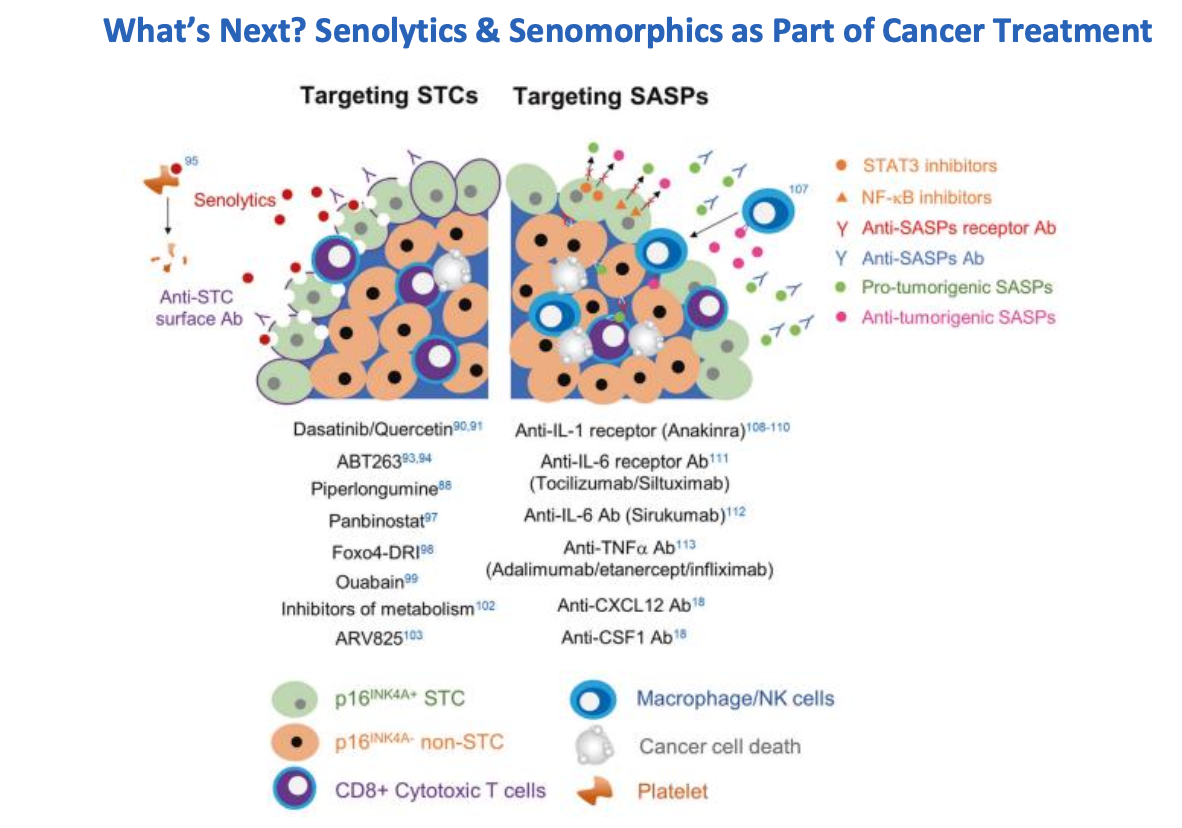
And I’ll jump to other aging biomarker news. And, you know, so this, I’m just gonna highlight, as many of you are probably already aware, Judy Campisi passed away very recently. She was a very well-known, respected aging researcher at the Buck Institute and, you know, and was involved. She was a rigorous researcher in the field when at a time where it was kind of academic suicide for many people to even enter the aging field. And so she’s really kind of a pioneer for everyone. And her work, of course, has been on cellular senescence, kind of the characterization of these zombie cells. And this figure is just describing how, you know, how they’re now very well characterized to suppress kind of tumors. But kind of the dark side is that while they, when cells turn senescent, they suppress tumors. They also impair tissue regeneration. They kind of lead to frailty. And she, in her lab, helped characterize the SASP, the senescence-associated secretory phenotype or profile, where there’s a lot of inflammatory cytokines that a lot of different types of inflammatory and maybe, you know, pro and non-inflammatory cytokines that are released by senescent cells and characterizing how, you know, what effects those have.
And one other comment about this is that, you know, her work has led to this field, you know, and senescence is a very well-accepted hallmark of aging. And there are now dozens of senolytic and cinnamorphic compounds that are available. And the area where I’m probably most excited about their use is in cancer treatment. And, you know, something, you know, I think more than 80% of cancers are carcinomas. And so they’re derived from epithelial tissue and where senescent cells build up over time. And I believe that, you know, I have a better understanding of senescent cells and kind of a testing of senolytics and cinnamorphics in kind of a precancerous or kind of neoadjuvant setting kind of after surgery where you’re removing solid tumors, you know, may end up to much better efficacy for treating those cancers. And, you know, and today, over 80% of cancers are carcinomas, like I mentioned, and there just aren’t that many good treatment options. You know, most of them have really, or many of them have really kind of awful three and five-year survival rates still. And so I’m kind of hopeful that’s what, you know, that’s a major impact that her work will have, you know, over the next decade. So improving outcomes in that area.
One other treatment, this is an in-the-pipeline treatment, meaning it’s an investigational agent. So it may not be available for five years or 10 years or longer, but this is a gut-related kind of intervention. And it really kind of speaks to how improving intestinal integrity, kind of intestinal permeability, or, you know, can improve, can have systemic benefits
. And they showed an improved survival and they showed, you know, a couple of other outcomes. So, you know, one of them also shown here is, you might be wondering what that picture is, but that’s a picture of rectal prolapse. So kind of an awful part of the aging process. You know, aging is not pretty, and that’s just another reminder, but their treatment was able to significantly reduce incidence in mice. And, you know, but, you know, it’s just that, I mean, there are many treatments like this in the pipeline, but, you know, we’re gonna focus mostly on treatments that are already available.
There were several papers and blogs that came out about rapamycin, and so I felt it would be useful just to look at some of the better publications that look at clinical data with it. And this paper came out from the CABRE line, and Alan Green, a physician, was involved with it. And it looks like it also has some of the AgelessRx group that was involved. But this is survey data. So they’re just polling people who took rapamycin off-label and trying to understand what the side effects are and what kind of benefits that people are seeing. And what they found or what they kind of reported from this survey study was that there actually weren’t that many prominent side effects. So the ones in green are where the controls actually had higher incidence of them than those who were treated on rapamycin. So these were not kind of side effects that we’re seeing. The only one that was higher in the rapamycin group were mouth ulcerations. But on the other hand, there weren’t the major subjective benefits seen of rapamycin treatment either. So these different surveys meant I’m happier, my brain works better, I have more energy. They were kind of in the 20% to 30% in general for people, 44% thought that their health had improved. Obviously, there are a lot of trials ongoing with rapamycin now. So there’s going to be a lot more objective data that’s obtained. This is a nice kind of survey. So with some subjective data on rapa’s benefits and side effects. This other paper just came out from Andrea Myers’ group, and it was a meta-analysis. And it was nice in that it looked at thousands of patients that were dosed with rapamycin and often at pretty high doses. So kind of much higher than the doses that are commonly used for rapamycin. So kind of you can see on the x-axis here, this is a weekly rapamycin dose. In some of these immune suppression studies, where they enroll healthy controls, they’re using the same dose per day. And even in those studies, they aren’t necessarily seeing really negative results in healthy controls. And I think this is kind of a nice figure also in that it shows many different doses that are used. And it’s also looking at different tissues and organ systems and kind of mapping with the green, yellow, and kind of red, whether or not there were positive or negative effects. And often there just weren’t any effects seen in healthy controls. But with lower doses, there were often kind of beneficial effects seen on different organ systems with rapamycin. And I’ll dig into a few different kinds of influencer or initiative updates. Often with the influencers, kind of people with podcasts, with blogs that have big followings, I often just like to kind of check, see what they’re saying. And if they release different lists of supplements they’re personally taking, maybe we can kind of put some of those to the test, launch our own studies. The XPRIZE had a big announcement in the last month or last, I think maybe actually it was November or December, but they announced their $101 million Healthspan XPRIZE. And it’s going to be a, so it’s a seven-year competition and they’re aiming to improve healthspan and they’re going to be focused on functional outcomes and trying to achieve a more than 10-year improvement of different functional outcomes. And they’re focused on muscle, the immune system, and on cognitive aging. So they’re trying to achieve more than a 10-year functional improvement in each of those areas. So there was this Twitter conversation, this just happened over the last few days, but I mean, it kind of gets at, I mean, a lot of gerontologists are on Twitter and they kind of argue back and forth and kind of this one thread came up, Matt Gaberlein, like kind of asked the question, has anybody really kind of reversed aging? And so people kind of jump in and David Sinclair, he actually quoted a results from a study that we did with a company, Rejuvenate Bio. I mean, Rejuvenate Bio led the study. It was on a systemic reprogramming model, and we did some clock testing for them. They extended the remaining lifespan by over 100%. Matt Gaberlein said that no one’s really reversed aging, but rapamycin does even better than that. It has more than a 100% extension of remaining lifespan, and caloric restriction does even better than rapamycin. The gist is that these are very semantic questions. It all revolves around what your definition of aging is or reversing aging. Certainly, this study we’ve seen definitely reversed epigenetic aging, and epigenetic aging is a very unbiased measure. But somebody like Matt Gaberlein or other gerontologists may say epigenetic aging isn’t the same as biological aging and it’s definitely not the same as actual aging. People will fight about it, but the promising part is that there are emerging studies like Rejuvenate 1 and more that are showing pretty clear results. This is a preprint, but it’s in peer review and they’re working pretty hard to get that out.
There is this initiative you may be familiar with, Aubrey de Grey, formerly of the SENS Foundation, now has this new group, the LEV Foundation, it’s Longevity Escape Velocity Foundation. They’re now doing mouse studies and looking at treatment combinations. One thing they found so far is that rapamycin and mTURT, so telomerase, extending telomere length, seem to be the most effective. They also find that treatment combinations work pretty well together and they’re still waiting on some more data to come in to really see what has the biggest benefit on max lifespan. But they just released results. The NIA has the Interventions Testing Program. These are mouse studies again, but it’s very rigorous testing of mouse lifespan where, for instance, they control for caloric restriction. Often, some of these preclinical studies don’t really control for that. So you can’t really tell, did the treatment have an effect or was it just dietary restriction? Was it just caloric restriction, which is kind of a gold standard longevity treatment that actually was at play? But they show that two treatments, astaxanthin, which is a carotenoid available in food and supplements, and also meclizine, which is dramamine. This kind of antihistamine agent, both of them had modest effects on healthspan and lifespan. And so that was a study that came out in the last couple of months from the ITP.
Finally, this is just a general science kind of off-topic, but there is somebody who posted about different classic academic papers that came out on why nature chose phosphates. There was this nice paper about modular biological complexity from Christoph Buck at Caltech, who’s done a lot of work on consciousness. But this is just a kind of general interest article, not a whole lot directly related to aging. But I thought I’d throw that in there. But that’s really the recap for this month, and I’m just going to take a look and see if we have any questions from that.
There were a couple of questions. They want your notes. They want you to share your notes. I said we’ll get that out. Yeah, we can put it out. And I know I have all these links in here that nobody can do anything with, right? We’ll send out a PDF of the slides for the recap, and you’ll be able to click the links at that point if you want. So a few questions. So any value in comparing methylation data with sequenced genomes, such as 23andMe, etc.? Yeah, definitely, in many studies, people are looking at genetic data with epigenetic data. And for instance, this paper that came out on causality-enriched clocks, what they’re often using is 40,000 samples, many genetic samples, from the UK Biobank. So they’re looking at genetic data in concert with epigenetic data. And they’re using this process known as Mendelian randomization to get at causal clocks, what modifications are driving epigenetic aging. That said, I think causal clocks will benefit most from interventional studies. We really need interventional studies that have clear effects on epigenetic clocks and functional outcomes before we can really understand what’s causal or not. But absolutely, Steve, there is a lot of value in combining genetic data with epigenetic data.
So Andre, you had mentioned what would be the driver to enable this. So there’s a question from Andre that mentions the price of methylation testing that I mentioned it’s possible to cut in half. What’s the driver to enable this? Is it purely volume? And custom chips or other effects as well? So yeah, this technology that I mentioned, it’s an entirely different kind of sequencing-based technology. And so there’s a few different groups working on this or techniques similar to this. So that would not use a custom chip. But what I was referring to in order to cut the cost in half by the end of the year is exactly what you’ve mentioned. It is a purely volume-based method where we have custom chips. And basically, if we can get 5,000 people or so to raise their hands and say, I’ll pay $150 for a test at the same time, then we would be able to commission a custom chip. And we’d be able to drive the price down significantly. So we’d be able to cut it in half. And we’re interested in doing that. And I think there might be a couple of people on the call that have been very supportive and that are helping to enable that. But we haven’t formally announced that initiative. But it is a pretty simple process. So in the benefit of using that method, it doesn’t get us down to under $100. But it may cut the pricing in half. And the real benefit is that it’s using a very proven technology, a very proven method. So we would get very reliable epigenetic clock data resulting from it. And again, about cutting half the cost.
And one question from John was, is anybody aware of human studies that correlate serum, clotho, SASP, metabolomics, and or epigenetics? There’s a lot of work from Riccardo Marioni’s lab in the UK where he’s doing multi-omic studies on large biobank populations. And often, I don’t know about clotho, but many of the SASP inflammatory cytokines, they’re used. And I think one of the papers that I put in here, the one on saliva-based methods with explainable protein episcores, that includes the Marioni group. But there are more papers from his lab, John. And that would be a good one to look at. He’s at the University of Edinburgh. And Steve, we don’t allow genetic data uploading right now. We just haven’t worked on it.
And the last question here, before we jump into the AKG segment, is that Alexander mentioned that a lot of his data, that aging is related to renewing bundles of cells. I mean, that’s kind of a loss of stem cells. And stem cell reservoirs are a well-accepted hallmark of aging. And they have an effect on epigenetic clocks. So stem cell reservoirs, stem cell pools, can definitely be measured with clocks. And so I think it is that they are pretty unbiased measures that enable measurement of it. But kind of the question is, are there studies that show how often after a treatment, somebody returns to their biological age? And that’s a really important question. Often these studies are done, and we’re going to talk about one in a second with AKG, where people are just doing a before and after. And they may even still be on treatment when they’re taking that second test. But really what we’re interested in are treatments where the effects are sustained, where they’re durable, where they’re long-term. And so we often, so I’ll often recommend to groups that you always include a follow-up time point. And it could be a time point, you know, three months after treatment stops or six months or a year. But often, you know, there are budgetary concerns. So it really depends on the treatment, but you absolutely, that’s a great question. You do always want to try to include follow-up time points.